Combating Pes Planus
Overview

Most people have a gap under the arch of their foot when they are in a standing position. The arch, the inner part of the foot is slightly raised off the ground. People with flat feet or fallen arches either have no arch, or it is very low. The feet of people with flat feet may roll over to the inner side when they are standing or walking, and the feet may point outwards as a result.
Causes
Footwear: shoes which limit toe movement; high heels. Barefoot walking may be protective. A tight Achilles tendon or calf muscles (heel cord contracture). This may help to cause Pes Planus, or may contribute to symptoms such as foot pain when there is existing Pes Planus. Obesity. Other bony abnormalities, eg rotational deformities, tibial abnormalities, coalition (fusion) of tarsal bones, equinus deformity. Ligamentous laxity, eg familial, Marfan's syndrome, Ehlers-Danlos syndrome, Down's syndrome. Other factors causing foot pronation, eg hip abductor weakness and genu valgum.
Symptoms
Symptoms that should be checked by a pediatrician include foot pain, sores or pressure areas on the inner side of the foot, a stiff foot, limited side-to-side foot motion, or limited up-and-down ankle motion. For further treatment you should see a pediatric orthopedic surgeon or podiatrist experienced in childhood foot conditions.
Diagnosis
Runners are often advised to get a gait analysis to determine what type of foot they have and so what kind of running shoe they require. This shouldn?t stop at runners. Anyone that plays sports could benefit from this assessment. Sports shoes such as football boots, astro trainers and squash trainers often have very poor arch support and so for the 60-80% of us who do overpronate or have flat feet they are left unsupported. A change of footwear or the insertion of arch support insoles or orthotics can make a massive difference to your risk of injury, to general aches and pains and even to your performance.
How do you get an arch in your foot?
Non Surgical Treatment
Most flexible flat feet are asymptomatic, and do not cause pain. In these cases, there is usually no cause for concern, and the condition may be considered a normal human variant. Flat feet were formerly a physical-health reason for service-rejection in many militaries. However, three military studies on asymptomatic adults (see section below), suggest that persons with asymptomatic flat feet are at least as tolerant of foot stress as the population with various grades of arch. Asymptomatic flat feet are no longer a service disqualification in the U.S. military.
Surgical Treatment

Common indications for surgery are cerebral palsy with an equinovalgus foot, to prevent progression and breakdown of the midfoot. Rigid and painful Pes Planus. To prevent progression, eg with a Charcot joint. Tibialis posterior dysfunction, where non-surgical treatment is unsuccessful. Possible surgical procedures include Achilles tendon lengthening. Calcaneal osteotomy, to re-align the hindfoot. Reconstruction of the tibialis posterior tendon. For severe midfoot collapse of the arch, triple arthrodesis may be indicated.
After Care
Time off work depends on the type of work as well as the surgical procedures performed. . A patient will be required to be non-weight bearing in a cast or splint and use crutches for four to twelve weeks. Usually a patient can return to work in one to two weeks if they are able to work while seated. If a person's job requires standing and walking, return to work may take several weeks. Complete recovery may take six months to a full year. Complications can occur as with all surgeries, but are minimized by strictly following your surgeon's post-operative instructions. The main complications include infection, bone that is slow to heal or does not heal, progression or reoccurrence of deformity, a stiff foot, and the need for further surgery. Many of the above complications can be avoided by only putting weight on the operative foot when allowed by your surgeon.
Most people have a gap under the arch of their foot when they are in a standing position. The arch, the inner part of the foot is slightly raised off the ground. People with flat feet or fallen arches either have no arch, or it is very low. The feet of people with flat feet may roll over to the inner side when they are standing or walking, and the feet may point outwards as a result.
Causes
Footwear: shoes which limit toe movement; high heels. Barefoot walking may be protective. A tight Achilles tendon or calf muscles (heel cord contracture). This may help to cause Pes Planus, or may contribute to symptoms such as foot pain when there is existing Pes Planus. Obesity. Other bony abnormalities, eg rotational deformities, tibial abnormalities, coalition (fusion) of tarsal bones, equinus deformity. Ligamentous laxity, eg familial, Marfan's syndrome, Ehlers-Danlos syndrome, Down's syndrome. Other factors causing foot pronation, eg hip abductor weakness and genu valgum.
Symptoms
Symptoms that should be checked by a pediatrician include foot pain, sores or pressure areas on the inner side of the foot, a stiff foot, limited side-to-side foot motion, or limited up-and-down ankle motion. For further treatment you should see a pediatric orthopedic surgeon or podiatrist experienced in childhood foot conditions.
Diagnosis
Runners are often advised to get a gait analysis to determine what type of foot they have and so what kind of running shoe they require. This shouldn?t stop at runners. Anyone that plays sports could benefit from this assessment. Sports shoes such as football boots, astro trainers and squash trainers often have very poor arch support and so for the 60-80% of us who do overpronate or have flat feet they are left unsupported. A change of footwear or the insertion of arch support insoles or orthotics can make a massive difference to your risk of injury, to general aches and pains and even to your performance.
How do you get an arch in your foot?
Non Surgical Treatment
Most flexible flat feet are asymptomatic, and do not cause pain. In these cases, there is usually no cause for concern, and the condition may be considered a normal human variant. Flat feet were formerly a physical-health reason for service-rejection in many militaries. However, three military studies on asymptomatic adults (see section below), suggest that persons with asymptomatic flat feet are at least as tolerant of foot stress as the population with various grades of arch. Asymptomatic flat feet are no longer a service disqualification in the U.S. military.
Surgical Treatment
Common indications for surgery are cerebral palsy with an equinovalgus foot, to prevent progression and breakdown of the midfoot. Rigid and painful Pes Planus. To prevent progression, eg with a Charcot joint. Tibialis posterior dysfunction, where non-surgical treatment is unsuccessful. Possible surgical procedures include Achilles tendon lengthening. Calcaneal osteotomy, to re-align the hindfoot. Reconstruction of the tibialis posterior tendon. For severe midfoot collapse of the arch, triple arthrodesis may be indicated.
After Care
Time off work depends on the type of work as well as the surgical procedures performed. . A patient will be required to be non-weight bearing in a cast or splint and use crutches for four to twelve weeks. Usually a patient can return to work in one to two weeks if they are able to work while seated. If a person's job requires standing and walking, return to work may take several weeks. Complete recovery may take six months to a full year. Complications can occur as with all surgeries, but are minimized by strictly following your surgeon's post-operative instructions. The main complications include infection, bone that is slow to heal or does not heal, progression or reoccurrence of deformity, a stiff foot, and the need for further surgery. Many of the above complications can be avoided by only putting weight on the operative foot when allowed by your surgeon.
Understand Heel Pain
Overview

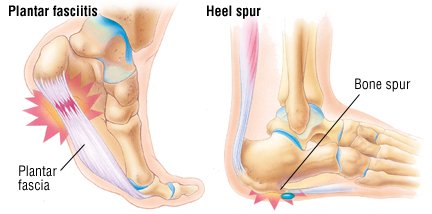
The most common cause of heel pain is plantar fasciitis which is commonly referred to as a heel spur. Plantar fascia is a broad band of fibrous tissue which runs along the bottom surface of the foot, from the heel to the toes. Plantar fasciitis is a condition in which the plantar fascia is inflamed. This condition can be very painful and cause a considerable amount of suffering.
Causes
Plantar fasciitis can come from a number of underlying causes. Finding the precise reason for the heel pain is sometimes difficult. As you can imagine, when the foot is on the ground a tremendous amount of force (the full weight of the body) is concentrated on the plantar fascia. This force stretches the plantar fascia as the arch of the foot tries to flatten from the weight of your body. This is just how the string on a bow is stretched by the force of the bow trying to straighten. This leads to stress on the plantar fascia where it attaches to the heel bone. Small tears of the fascia can result. These tears are normally repaired by the body. As this process of injury and repair repeats itself over and over again, a bone spur (a pointed outgrowth of the bone) sometimes forms as the body's response to try to firmly attach the fascia to the heelbone. This appears on an X-ray of the foot as a heel spur. Bone spurs occur along with plantar fasciitis but they are not the cause of the problem. As we age, the very important fat pad that makes up the fleshy portion of the heel becomes thinner and degenerates (starts to break down). This can lead to inadequate padding on the heel. With less of a protective pad on the heel, there is a reduced amount of shock absorption. These are additional factors that might lead to plantar fasciitis. Some physicians feel that the small nerves that travel under the plantar fascia on their way to the forefoot become irritated and may contribute to the pain. But some studies have been able to show that pain from compression of the nerve is different from plantar fasciitis pain. In many cases, the actual source of the painful heel may not be defined clearly. Other factors that may contribute to the development of plantar fasciitis include obesity, trauma, weak plantar flexor muscles, excessive foot pronation (flat foot) or other alignment problems in the foot and or ankle, and poor footwear.
Symptoms
Symptoms of plantar fasciitis vary, but the classic symptom is pain after rest--when you first get out of bed in the morning, or when you get up after sitting down for a while during the day. The pain usually diminishes after a few minutes of walking, sometimes even disappearing, but the pain is commonly felt again the longer you're on the foot. Fasciitis can be aggravated by shoes that lack appropriate support, especially in the arch area, and by the chronic irritation of long-periods of standing, especially on concrete, by being overweight. It doesn't help that fascia doesn't heal particularly quickly because it has relatively poor circulation (which is why it's white in colour).
Diagnosis
Your doctor will perform a physical exam and ask questions about your medical history and symptoms, such as have you had this type of heel pain before? When did your pain begin? Do you have pain upon your first steps in the morning or after your first steps after rest? Is the pain dull and aching or sharp and stabbing? Is it worse after exercise? Is it worse when standing? Did you fall or twist your ankle recently? Are you a runner? If so, how far and how often do you run? Do you walk or stand for long periods of time? What kind of shoes do you wear? Do you have any other symptoms? Your doctor may order a foot x-ray. You may need to see a physical therapist to learn exercises to stretch and strengthen your foot. Your doctor may recommend a night splint to help stretch your foot. Surgery may be recommended in some cases.
Non Surgical Treatment
If you develop heel pain, you can try several methods at home to ease your discomfort. For example rest as much as possible, apply ice to the heel for 10 to 15 minutes twice a day, use over-the-counter pain medications, wear shoes that fit properly, wear night splints, a special device that stretches the foot while you sleep, use heel cups or shoe inserts to reduce pain, If these home care strategies do not ease your pain, you will need to see your doctor. He or she will perform a physical exam and ask you about your symptoms and when they began. Your doctor may also take an X-ray to determine the cause of your heel pain. Once your doctor knows what is causing your pain, he or she will be able to provide you with the appropriate treatment. In many cases, your doctor may prescribe physical therapy. This can help to strengthen the muscles and tendons in your foot, which helps to prevent further injury. If your pain is severe, your doctor may provide you with anti-inflammatory medications. These medications can be injected into the foot or taken by mouth. Your doctor may also recommend that you support your foot as much as possible-either by taping the foot or by using special footwear devices. In very rare cases, your doctor may recommend surgery to correct the problem. However, heel surgery often requires a long recovery time and may not always relieve your foot pain.
Surgical Treatment
Only a relatively few cases of heel pain require surgery. If required, surgery is usually for the removal of a spur, but also may involve release of the plantar fascia, removal of a bursa, or a removal of a neuroma or other soft-tissue growth.
bestshoelifts
Prevention
It is not always possible to prevent heel pain, but there are measures you can take to help avoid further episodes. Being overweight can place excess pressure and strain on your feet, particularly on your heels. This increases the risk of damaging your feet and heels. If you are overweight, losing weight and maintaining a healthy weight by combining regular exercise with a healthy, balanced diet can be beneficial for your feet. You can calculate your body mass index (BMI) to find out whether you are a healthy weight for your height and build. To work out your BMI, divide your weight in kilograms by your height in metres squared. A BMI of less than 18.5 means that you are underweight, 18.5-24.9 means that your weight is healthy, 25-29 means that you are overweight, 30-40 means that you are obese, over 40 means that you are morbidly obese. You can also use the BMI healthy weight calculator to work out your BMI.
The most common cause of heel pain is plantar fasciitis which is commonly referred to as a heel spur. Plantar fascia is a broad band of fibrous tissue which runs along the bottom surface of the foot, from the heel to the toes. Plantar fasciitis is a condition in which the plantar fascia is inflamed. This condition can be very painful and cause a considerable amount of suffering.
Causes
Plantar fasciitis can come from a number of underlying causes. Finding the precise reason for the heel pain is sometimes difficult. As you can imagine, when the foot is on the ground a tremendous amount of force (the full weight of the body) is concentrated on the plantar fascia. This force stretches the plantar fascia as the arch of the foot tries to flatten from the weight of your body. This is just how the string on a bow is stretched by the force of the bow trying to straighten. This leads to stress on the plantar fascia where it attaches to the heel bone. Small tears of the fascia can result. These tears are normally repaired by the body. As this process of injury and repair repeats itself over and over again, a bone spur (a pointed outgrowth of the bone) sometimes forms as the body's response to try to firmly attach the fascia to the heelbone. This appears on an X-ray of the foot as a heel spur. Bone spurs occur along with plantar fasciitis but they are not the cause of the problem. As we age, the very important fat pad that makes up the fleshy portion of the heel becomes thinner and degenerates (starts to break down). This can lead to inadequate padding on the heel. With less of a protective pad on the heel, there is a reduced amount of shock absorption. These are additional factors that might lead to plantar fasciitis. Some physicians feel that the small nerves that travel under the plantar fascia on their way to the forefoot become irritated and may contribute to the pain. But some studies have been able to show that pain from compression of the nerve is different from plantar fasciitis pain. In many cases, the actual source of the painful heel may not be defined clearly. Other factors that may contribute to the development of plantar fasciitis include obesity, trauma, weak plantar flexor muscles, excessive foot pronation (flat foot) or other alignment problems in the foot and or ankle, and poor footwear.
Symptoms
Symptoms of plantar fasciitis vary, but the classic symptom is pain after rest--when you first get out of bed in the morning, or when you get up after sitting down for a while during the day. The pain usually diminishes after a few minutes of walking, sometimes even disappearing, but the pain is commonly felt again the longer you're on the foot. Fasciitis can be aggravated by shoes that lack appropriate support, especially in the arch area, and by the chronic irritation of long-periods of standing, especially on concrete, by being overweight. It doesn't help that fascia doesn't heal particularly quickly because it has relatively poor circulation (which is why it's white in colour).
Diagnosis
Your doctor will perform a physical exam and ask questions about your medical history and symptoms, such as have you had this type of heel pain before? When did your pain begin? Do you have pain upon your first steps in the morning or after your first steps after rest? Is the pain dull and aching or sharp and stabbing? Is it worse after exercise? Is it worse when standing? Did you fall or twist your ankle recently? Are you a runner? If so, how far and how often do you run? Do you walk or stand for long periods of time? What kind of shoes do you wear? Do you have any other symptoms? Your doctor may order a foot x-ray. You may need to see a physical therapist to learn exercises to stretch and strengthen your foot. Your doctor may recommend a night splint to help stretch your foot. Surgery may be recommended in some cases.
Non Surgical Treatment
If you develop heel pain, you can try several methods at home to ease your discomfort. For example rest as much as possible, apply ice to the heel for 10 to 15 minutes twice a day, use over-the-counter pain medications, wear shoes that fit properly, wear night splints, a special device that stretches the foot while you sleep, use heel cups or shoe inserts to reduce pain, If these home care strategies do not ease your pain, you will need to see your doctor. He or she will perform a physical exam and ask you about your symptoms and when they began. Your doctor may also take an X-ray to determine the cause of your heel pain. Once your doctor knows what is causing your pain, he or she will be able to provide you with the appropriate treatment. In many cases, your doctor may prescribe physical therapy. This can help to strengthen the muscles and tendons in your foot, which helps to prevent further injury. If your pain is severe, your doctor may provide you with anti-inflammatory medications. These medications can be injected into the foot or taken by mouth. Your doctor may also recommend that you support your foot as much as possible-either by taping the foot or by using special footwear devices. In very rare cases, your doctor may recommend surgery to correct the problem. However, heel surgery often requires a long recovery time and may not always relieve your foot pain.
Surgical Treatment
Only a relatively few cases of heel pain require surgery. If required, surgery is usually for the removal of a spur, but also may involve release of the plantar fascia, removal of a bursa, or a removal of a neuroma or other soft-tissue growth.
bestshoelifts
Prevention
It is not always possible to prevent heel pain, but there are measures you can take to help avoid further episodes. Being overweight can place excess pressure and strain on your feet, particularly on your heels. This increases the risk of damaging your feet and heels. If you are overweight, losing weight and maintaining a healthy weight by combining regular exercise with a healthy, balanced diet can be beneficial for your feet. You can calculate your body mass index (BMI) to find out whether you are a healthy weight for your height and build. To work out your BMI, divide your weight in kilograms by your height in metres squared. A BMI of less than 18.5 means that you are underweight, 18.5-24.9 means that your weight is healthy, 25-29 means that you are overweight, 30-40 means that you are obese, over 40 means that you are morbidly obese. You can also use the BMI healthy weight calculator to work out your BMI.
Leg Length Discrepancy Shoe Wear Pattern
Overview
The majority of people in the world actually have some degree of leg length discrepancy, up to 2cm. One study found that only around 1/4 of people have legs of equal lengths. LLD of greater than 2cm is relatively rare, however, and the greater the discrepancy, the greater the chances of having a clinical problem down the road. A limp generally begins when LLD exceeds 2cm and becomes extremely noticeable above 3cm. When patients with LLD develop an abnormal gait, one of the debilitating clinical features can be fatigue because of the relatively high amount of energy needed to walk in the new, inefficient way. Poliomyelitis, or polio, as it is more commonly known, used to account for around 1/3 of all cases of LLD, but due to the effectiveness of polio vaccines, it now represents a negligible cause of the condition. Functional LLD, described above, usually involves treatment focused on the hip, pelvis, and/or lower back, rather than the leg. If you have been diagnosed with functional LLD or pelvic obliquity, please ask your orthopaedic surgeon for more information about treatment of these conditions.
Causes
The causes of LLD may be divided into those that shorten a limb versus those that lengthen a limb, or they may be classified as affecting the length versus the rate of growth in a limb. For example, a fracture that heals poorly may shorten a leg slightly, but does not affect its growth rate. Radiation, on the other hand, can affect a leg's long-term ability to expand, but does not acutely affect its length. Causes that shorten the leg are more common than those that lengthen it and include congenital growth deficiencies (seen in hemiatrophy and skeletal dysplasias ), infections that infiltrate the epiphysis (e.g. osteomyelitis ), tumors, fractures that occur through the growth plate or have overriding ends, Legg-Calve-Perthes disease, slipped capital femoral epiphysis (SCFE), and radiation. Lengthening can result from unique conditions, such as hemihypertrophy , in which one or more structures on one side of the body become larger than the other side, vascular malformations or tumors (such as hemangioma ), which cause blood flow on one side to exceed that of the other, Wilm's tumor (of the kidney), septic arthritis, healed fractures, or orthopaedic surgery. Leg length discrepancy may arise from a problem in almost any portion of the femur or tibia. For example, fractures can occur at virtually all levels of the two bones. Fractures or other problems of the fibula do not lead to LLD, as long as the more central, weight-bearing tibia is unaffected. Because many cases of LLD are due to decreased rate of growth, the femoral or tibial epiphyses are commonly affected regions.
Symptoms
Back pain along with pain in the foot, knee, leg and hip on one side of the body are the main complaints. There may also be limping or head bop down on the short side or uneven arm swinging. The knee bend, hip or shoulder may be down on one side, and there may be uneven wear to the soles of shoes (usually more on the longer side).
Diagnosis
Limb length discrepancy can be measured by a physician during a physical examination and through X-rays. Usually, the physician measures the level of the hips when the child is standing barefoot. A series of measured wooden blocks may be placed under the short leg until the hips are level. If the physician believes a more precise measurement is needed, he or she may use X-rays. In growing children, a physician may repeat the physical examination and X-rays every six months to a year to see if the limb length discrepancy has increased or remained unchanged. A limb length discrepancy may be detected on a screening examination for curvature of the spine (scoliosis). But limb length discrepancy does not cause scoliosis.
Non Surgical Treatment
Treatment of leg length inequality involves many different approaches, which vary among osteopaths, physiotherapist and chiropractor and whether the LLD is functional or structural. Thus is a combination of myofascial release (massage) & stretching of shortened muscles. Manipulation or mobilization of the spine, sacro-iliac joint (SIJ), hip, knee, foot. Orthotics, shoe lifts can be used to treat discrepancies from two to six cm (usually up to 1 cm can be inserted in the shoe. For larger leg length inequalities, the shoe must be built up. This needs to be done for every shoe worn, thus limiting the type of shoe that the patient can wear). Surgery (epiphysiodesis, epiphyseal stapling,bone resection).

can you stretch to get taller?
Surgical Treatment
Surgical options in leg length discrepancy treatment include procedures to lengthen the shorter leg, or shorten the longer leg. Your child's physician will choose the safest and most effective method based on the aforementioned factors. No matter the surgical procedure performed, physical therapy will be required after surgery in order to stretch muscles and help support the flexibility of the surrounding joints. Surgical shortening is safer than surgical lengthening and has fewer complications. Surgical procedures to shorten one leg include removing part of a bone, called a bone resection. They can also include epiphysiodesis or epiphyseal stapling, where the growth plate in a bone is tethered or stapled. This slows the rate of growth in the surgical leg.
The majority of people in the world actually have some degree of leg length discrepancy, up to 2cm. One study found that only around 1/4 of people have legs of equal lengths. LLD of greater than 2cm is relatively rare, however, and the greater the discrepancy, the greater the chances of having a clinical problem down the road. A limp generally begins when LLD exceeds 2cm and becomes extremely noticeable above 3cm. When patients with LLD develop an abnormal gait, one of the debilitating clinical features can be fatigue because of the relatively high amount of energy needed to walk in the new, inefficient way. Poliomyelitis, or polio, as it is more commonly known, used to account for around 1/3 of all cases of LLD, but due to the effectiveness of polio vaccines, it now represents a negligible cause of the condition. Functional LLD, described above, usually involves treatment focused on the hip, pelvis, and/or lower back, rather than the leg. If you have been diagnosed with functional LLD or pelvic obliquity, please ask your orthopaedic surgeon for more information about treatment of these conditions.
Causes
The causes of LLD may be divided into those that shorten a limb versus those that lengthen a limb, or they may be classified as affecting the length versus the rate of growth in a limb. For example, a fracture that heals poorly may shorten a leg slightly, but does not affect its growth rate. Radiation, on the other hand, can affect a leg's long-term ability to expand, but does not acutely affect its length. Causes that shorten the leg are more common than those that lengthen it and include congenital growth deficiencies (seen in hemiatrophy and skeletal dysplasias ), infections that infiltrate the epiphysis (e.g. osteomyelitis ), tumors, fractures that occur through the growth plate or have overriding ends, Legg-Calve-Perthes disease, slipped capital femoral epiphysis (SCFE), and radiation. Lengthening can result from unique conditions, such as hemihypertrophy , in which one or more structures on one side of the body become larger than the other side, vascular malformations or tumors (such as hemangioma ), which cause blood flow on one side to exceed that of the other, Wilm's tumor (of the kidney), septic arthritis, healed fractures, or orthopaedic surgery. Leg length discrepancy may arise from a problem in almost any portion of the femur or tibia. For example, fractures can occur at virtually all levels of the two bones. Fractures or other problems of the fibula do not lead to LLD, as long as the more central, weight-bearing tibia is unaffected. Because many cases of LLD are due to decreased rate of growth, the femoral or tibial epiphyses are commonly affected regions.
Symptoms
Back pain along with pain in the foot, knee, leg and hip on one side of the body are the main complaints. There may also be limping or head bop down on the short side or uneven arm swinging. The knee bend, hip or shoulder may be down on one side, and there may be uneven wear to the soles of shoes (usually more on the longer side).
Diagnosis
Limb length discrepancy can be measured by a physician during a physical examination and through X-rays. Usually, the physician measures the level of the hips when the child is standing barefoot. A series of measured wooden blocks may be placed under the short leg until the hips are level. If the physician believes a more precise measurement is needed, he or she may use X-rays. In growing children, a physician may repeat the physical examination and X-rays every six months to a year to see if the limb length discrepancy has increased or remained unchanged. A limb length discrepancy may be detected on a screening examination for curvature of the spine (scoliosis). But limb length discrepancy does not cause scoliosis.
Non Surgical Treatment
Treatment of leg length inequality involves many different approaches, which vary among osteopaths, physiotherapist and chiropractor and whether the LLD is functional or structural. Thus is a combination of myofascial release (massage) & stretching of shortened muscles. Manipulation or mobilization of the spine, sacro-iliac joint (SIJ), hip, knee, foot. Orthotics, shoe lifts can be used to treat discrepancies from two to six cm (usually up to 1 cm can be inserted in the shoe. For larger leg length inequalities, the shoe must be built up. This needs to be done for every shoe worn, thus limiting the type of shoe that the patient can wear). Surgery (epiphysiodesis, epiphyseal stapling,bone resection).
can you stretch to get taller?
Surgical Treatment
Surgical options in leg length discrepancy treatment include procedures to lengthen the shorter leg, or shorten the longer leg. Your child's physician will choose the safest and most effective method based on the aforementioned factors. No matter the surgical procedure performed, physical therapy will be required after surgery in order to stretch muscles and help support the flexibility of the surrounding joints. Surgical shortening is safer than surgical lengthening and has fewer complications. Surgical procedures to shorten one leg include removing part of a bone, called a bone resection. They can also include epiphysiodesis or epiphyseal stapling, where the growth plate in a bone is tethered or stapled. This slows the rate of growth in the surgical leg.
What Is Mortons Neuroma
Overview
 Morton's Neuroma is the most common neuroma in the foot. It occurs in the forefoot area (the ball of the foot) at the base of the third and fourth toes. It is sometimes referred to as an intermetatarsal neuroma. "Intermetatarsal" describes its location in the ball of the foot between the metatarsal bones (the bones extending from the toes to the midfoot). A neuroma is a thickening, or enlargement, of the nerve as a result of compression or irritation of the nerve. Compression and irritation creates swelling of the nerve, which can eventually lead to permanent nerve damage.
Morton's Neuroma is the most common neuroma in the foot. It occurs in the forefoot area (the ball of the foot) at the base of the third and fourth toes. It is sometimes referred to as an intermetatarsal neuroma. "Intermetatarsal" describes its location in the ball of the foot between the metatarsal bones (the bones extending from the toes to the midfoot). A neuroma is a thickening, or enlargement, of the nerve as a result of compression or irritation of the nerve. Compression and irritation creates swelling of the nerve, which can eventually lead to permanent nerve damage.
Causes
Although in many areas of medicine, it?s easy to pinpoint the exact source of a problem (the way a specific germ causes a certain illness with recognizable symptoms), neuromas are harder to categorize. While there isn?t really one exact cause, podiatric physicians tend to agree that a neuroma can occur in response to the irritation of a nerve by one or more factors. Abnormality in foot function or foot mechanics: In other words, a foot that doesn?t move the way science thinks it should. In general, this means a pronated foot (one with an excessive rolling motion when the patient is walking, running or doing any kind of activity), because it causes excessive strain on the nerve. If you are not certain whether or not this is a problem for you, ask your podiatric physician, who will be able to examine your feet, as well as the wear pattern on your shoe, and give you an answer. Foot mechanics, and problems with them, tend to run in families, so if you know that a relative has had foot pain similar to yours, be sure to mention it.
Symptoms
Symptoms associated with a neuroma include a dull burning sensation radiating towards the toes, a cramping feeling, or even a stinging, tingling sensation that can be described as being similar to an electric shock. It is often worse when wearing shoes with most people finding the pain disappears when removing their shoes.
Diagnosis
Morton's neuroma is usually diagnosed by your doctor listening to your symptoms and examining your foot. Sometimes your doctor can feel the 'neuroma', or an area of thickening in your foot, which may be tender. Sometimes, your doctor may suggest an ultrasound scan or MRI scan to confirm the diagnosis but this is not always necessary. Some doctors inject a local anaesthetic into the area where you are experiencing pain. If this causes temporary relief of pain, burning and tingling, it can sometimes help to confirm the diagnosis and show the doctor where the problem is.
Non Surgical Treatment
Properly resting the foot in addition to the use of appropriate footwear including, as necessary, pads and arch supports, often brings relief from Morton?s Neuroma, without resorting to surgery. A physician may also recommend anti-inflammatory drugs, cortisone injections and, should the condition fail to resolve itself, surgery.
Surgical Treatment
Surgery for Morton's neuroma is usually a treatment of last resort. It may be recommended if you have severe pain in your foot or if non-surgical treatments haven't worked. Surgery is usually carried out under local anaesthetic, on an outpatient basis, which means you won't need to stay in hospital overnight. The operation can take up to 30 minutes. The surgeon will make a small incision, either on the top of your foot or on the sole. They may try to increase the space around the nerve (nerve decompression) by removing some of the surrounding tissue, or they may remove the nerve completely (nerve resection). If the nerve is removed, the area between your toes may be permanently numb. After the procedure you'll need to wear a special protective shoe until the affected area has healed sufficiently to wear normal footwear. It can take up to four weeks to make a full recovery. Most people (about 75%) who have surgery to treat Morton's neuroma have positive results and their painful symptoms are relieved.
Morton's Neuroma is the most common neuroma in the foot. It occurs in the forefoot area (the ball of the foot) at the base of the third and fourth toes. It is sometimes referred to as an intermetatarsal neuroma. "Intermetatarsal" describes its location in the ball of the foot between the metatarsal bones (the bones extending from the toes to the midfoot). A neuroma is a thickening, or enlargement, of the nerve as a result of compression or irritation of the nerve. Compression and irritation creates swelling of the nerve, which can eventually lead to permanent nerve damage.Causes
Although in many areas of medicine, it?s easy to pinpoint the exact source of a problem (the way a specific germ causes a certain illness with recognizable symptoms), neuromas are harder to categorize. While there isn?t really one exact cause, podiatric physicians tend to agree that a neuroma can occur in response to the irritation of a nerve by one or more factors. Abnormality in foot function or foot mechanics: In other words, a foot that doesn?t move the way science thinks it should. In general, this means a pronated foot (one with an excessive rolling motion when the patient is walking, running or doing any kind of activity), because it causes excessive strain on the nerve. If you are not certain whether or not this is a problem for you, ask your podiatric physician, who will be able to examine your feet, as well as the wear pattern on your shoe, and give you an answer. Foot mechanics, and problems with them, tend to run in families, so if you know that a relative has had foot pain similar to yours, be sure to mention it.
Symptoms
Symptoms associated with a neuroma include a dull burning sensation radiating towards the toes, a cramping feeling, or even a stinging, tingling sensation that can be described as being similar to an electric shock. It is often worse when wearing shoes with most people finding the pain disappears when removing their shoes.
Diagnosis
Morton's neuroma is usually diagnosed by your doctor listening to your symptoms and examining your foot. Sometimes your doctor can feel the 'neuroma', or an area of thickening in your foot, which may be tender. Sometimes, your doctor may suggest an ultrasound scan or MRI scan to confirm the diagnosis but this is not always necessary. Some doctors inject a local anaesthetic into the area where you are experiencing pain. If this causes temporary relief of pain, burning and tingling, it can sometimes help to confirm the diagnosis and show the doctor where the problem is.
Non Surgical Treatment
Properly resting the foot in addition to the use of appropriate footwear including, as necessary, pads and arch supports, often brings relief from Morton?s Neuroma, without resorting to surgery. A physician may also recommend anti-inflammatory drugs, cortisone injections and, should the condition fail to resolve itself, surgery.
Surgical Treatment
Surgery for Morton's neuroma is usually a treatment of last resort. It may be recommended if you have severe pain in your foot or if non-surgical treatments haven't worked. Surgery is usually carried out under local anaesthetic, on an outpatient basis, which means you won't need to stay in hospital overnight. The operation can take up to 30 minutes. The surgeon will make a small incision, either on the top of your foot or on the sole. They may try to increase the space around the nerve (nerve decompression) by removing some of the surrounding tissue, or they may remove the nerve completely (nerve resection). If the nerve is removed, the area between your toes may be permanently numb. After the procedure you'll need to wear a special protective shoe until the affected area has healed sufficiently to wear normal footwear. It can take up to four weeks to make a full recovery. Most people (about 75%) who have surgery to treat Morton's neuroma have positive results and their painful symptoms are relieved.
The Best Solution To Leg Length Imbalances Are Shoe Lifts
There are actually not one but two different types of leg length discrepancies, congenital and acquired. Congenital indicates that you are born with it. One leg is structurally shorter than the other. Through developmental periods of aging, the human brain senses the step pattern and recognizes some difference. The human body usually adapts by tilting one shoulder to the "short" side. A difference of less than a quarter inch isn't really excessive, require Shoe Lifts to compensate and normally does not have a serious effect over a lifetime.

Leg length inequality goes largely undiagnosed on a daily basis, however this condition is easily remedied, and can eliminate a number of cases of low back pain.
Treatment for leg length inequality typically consists of Shoe Lifts. These are typically low cost, regularly costing less than twenty dollars, compared to a custom orthotic of $200 plus. Differences over a quarter inch can take their toll on the spine and should probably be compensated for with a heel lift. In some cases, the shortage can be so extreme that it requires a full lift to both the heel and sole of the shoe.
Back ache is easily the most prevalent ailment afflicting men and women today. Around 80 million people suffer from back pain at some stage in their life. It is a problem that costs employers millions annually as a result of time lost and productivity. Innovative and better treatment solutions are always sought after in the hope of minimizing the economic impact this condition causes.

Men and women from all corners of the world suffer the pain of foot ache due to leg length discrepancy. In most of these cases Shoe Lifts can be of very helpful. The lifts are capable of easing any discomfort and pain in the feet. Shoe Lifts are recommended by many skilled orthopaedic orthopedists.
So that they can support the human body in a well balanced manner, your feet have a critical role to play. Irrespective of that, it is often the most neglected region of the body. Some people have flat-feet which means there may be unequal force exerted on the feet. This will cause other parts of the body such as knees, ankles and backs to be impacted too. Shoe Lifts ensure that suitable posture and balance are restored.
Leg length inequality goes largely undiagnosed on a daily basis, however this condition is easily remedied, and can eliminate a number of cases of low back pain.
Treatment for leg length inequality typically consists of Shoe Lifts. These are typically low cost, regularly costing less than twenty dollars, compared to a custom orthotic of $200 plus. Differences over a quarter inch can take their toll on the spine and should probably be compensated for with a heel lift. In some cases, the shortage can be so extreme that it requires a full lift to both the heel and sole of the shoe.
Back ache is easily the most prevalent ailment afflicting men and women today. Around 80 million people suffer from back pain at some stage in their life. It is a problem that costs employers millions annually as a result of time lost and productivity. Innovative and better treatment solutions are always sought after in the hope of minimizing the economic impact this condition causes.
Men and women from all corners of the world suffer the pain of foot ache due to leg length discrepancy. In most of these cases Shoe Lifts can be of very helpful. The lifts are capable of easing any discomfort and pain in the feet. Shoe Lifts are recommended by many skilled orthopaedic orthopedists.
So that they can support the human body in a well balanced manner, your feet have a critical role to play. Irrespective of that, it is often the most neglected region of the body. Some people have flat-feet which means there may be unequal force exerted on the feet. This will cause other parts of the body such as knees, ankles and backs to be impacted too. Shoe Lifts ensure that suitable posture and balance are restored.
Identifying Inferior Calcaneal Spur

Overview
Heel spurs occur in at least half the people who have plantar fasciitis, a painful condition involving the thick tissue that runs between your heel bone and your toes. In the past, doctors often performed surgery to remove heel spurs, believing them to be the cause of the pain associated with plantar fasciitis. In treating plantar fasciitis now, doctors rely more on ice, arch supports, physical therapy and pain medications, and surgery is rarely performed.
Causes
Heel spurs are exacerbated by an movements that stretch, twist or impact the plantar ligaments. Running, jumping, standing or walking on hard surfaces with unsupportive shoes, walking barefoot in sand are all activities that can activate heel spurs and plantar fasciitis. Obesity is another factor that increases stress to the plantar ligaments.

Symptoms
Symptoms of heel spur syndrome often include pain early in the morning or after rest, as you take the first few steps. It may also include severe pain after standing or walking long hours, especially on hard cement floors. Usually more pain exist while wearing a very flat soled shoe. A higher heel may actually relieve the pain as an arch is created. The pain is usually sharp, but can also be a dull ache. The pain may only be at the bottom of the heel, or may also travel along the arch of the foot.
Diagnosis
Diagnosis of a heel spur can be done with an x-ray, which will be able to reveal the bony spur. Normally, it occurs where the plantar fascia connects to the heel bone. When the plantar fascia ligament is pulled excessively it begins to pull away from the heel bone. When this excessive pulling occurs, it causes the body to respond by depositing calcium in the injured area, resulting in the formation of the bone spur. The Plantar fascia ligament is a fibrous band of connective tissue running between the heel bone and the ball of the foot. This structure maintains the arch of the foot and distributes weight along the foot as we walk. However, due to the stress that this ligament must endure, it can easily become damaged which commonly occurs along with heel spurs.
Non Surgical Treatment
A conventional treatment for a heel spur is a steroid injection. This treatment, however, isn?t always effective because of the many structures in the heel, making it a difficult place for an injection. If this treatment goes wrong, it can make the original symptoms even worse. Another interesting means of treatment is Cryoultrasound, an innovative electromedical device that utilizes the combination of two therapeutic techniques: cryotherapy and ultrasound therapy. Treatments with Cryoultrasound accelerate the healing process by interrupting the cycle and pain and spasms. This form of therapy increases blood circulation and cell metabolism; it stimulates toxin elimination and is supposed to speed up recovery.
Surgical Treatment
More than 90 percent of people get better with nonsurgical treatments. If conservative treatment fails to treat symptoms of heel spurs after a period of 9 to 12 months, surgery may be necessary to relieve pain and restore mobility. Surgical techniques include release of the plantar fascia, removal of a spur. Pre-surgical tests or exams are required to identify optimal candidates, and it's important to observe post-surgical recommendations concerning rest, ice, compression, elevation of the foot, and when to place weight on the operated foot. In some cases, it may be necessary for patients to use bandages, splints, casts, surgical shoes, crutches, or canes after surgery. Possible complications of heel surgery include nerve pain, recurrent heel pain, permanent numbness of the area, infection, and scarring. In addition, with plantar fascia release, there is risk of instability, foot cramps, stress fracture, and tendinitis.
The Right Way To Treat Inferior Calcaneal Spur

Overview
Bone spurs usually form around joints that have arthritis, in the vertebrae of the spine, and on the heel. When they form on the heel, they may form on the back of the heel but usually form on the bottom of the heel. Of course, this is where all of the body weight comes down with each step. Spurs on the bottom of the heel are usually most painful the first few steps out of bed each morning. The pain may lessen somewhat after walking for a few minutes, but may be intense again after sitting for a half hour or so, such as after lunch. The pain usually gets worse throughout the day as you are up on your feet more. Often the pain feels like a nail being driven through the heel into the ankle and leg.
Causes
One of the most common causes for the development of heel spurs is the wearing of shoes that are too tight. That?s why more women suffer from heel spurs more than men. Athletes who tend to stress their feet a lot, people are overweight who have more pressure on their lower extremities and the elderly also tend to suffer more from heel spurs.

Symptoms
If your body has created calcium build-ups in an effort to support your plantar fascia ligament, each time you step down with your foot, the heel spur is being driven into the soft, fatty tissue which lines the bottom of your heel. Heel spur sufferers experience stabbing sensations because the hard protrusion is literally being jabbed into the heel pad. If left untreated, Plantar Fasciitis and heel spurs can erode the fatty pad of the heel and cause permanent damage to the foot. Fortunately, most cases can be resolved without medications or surgeries.
Diagnosis
A thorough medical history and physical exam by a physician is always necessary for the proper diagnosis of heel spurs and other foot conditions. X rays of the heel area are helpful, as excess bone production will be visible.
Non Surgical Treatment
Heel pain may be associated with a heel spur, however the heel pain is usually due to plantar fasciitis, rather than a heel spur, so treatment is usually directed at the plantar fasciitis itself. Treatment usually involves application of ice to reduce pain and inflammation, special stretching exercises, and pain-relieving or anti-inflammatory medicines. Night splints or orthotics may be recommended. It may help to avoid the activities that aggravate pain, such as long walks and running. Surgery is very rarely recommended and only after other measures fail.
Surgical Treatment
Surgery involves releasing a part of the plantar fascia from its insertion in the heel bone, as well as removing the spur. Many times during the procedure, pinched nerves (neuromas), adding to the pain, are found and removed. Often, an inflamed sac of fluid call an accessory or adventitious bursa is found under the heel spur, and it is removed as well. Postoperative recovery is usually a slipper cast and minimal weight bearing for a period of 3-4 weeks. On some occasions, a removable short-leg walking boot is used or a below knee cast applied.
Prevention
o help prevent heel and bone spurs, wear properly designed and fitted shoes or boots that provide sufficient room in the toe box so as not to compress the toes. They should also provide cushioning in appropriate areas to minimize the possibility of the irritation and inflammation that can lead to bone spurs in the feet. If needed, use inserts that provide arch support and a slight heel lift to help ensure that not too much stress is placed on the plantar fascia. This helps to reduce the possibility of inflammation and overstress. Wearing padded socks can also help by reducing trauma. Peer-reviewed, published studies have shown that wearing clinically-tested padded socks can help protect against injuries to the skin/soft tissue of the foot due to the effects of impact, pressure and shear forces. Also consider getting your gait analyzed by a foot health professional for appropriate orthotics. If you have heel pain, toe pain or top-of-the-foot pain, see your doctor or foot specialist to ensure that a spur has not developed.